In this prospective cohort study, resistance training among US adult health care professionals was associated with substantially lower T2D risk, particularly when performed consistently over midlife and combined with adequate aerobic activity and limited sedentary television viewing. These findings support the inclusion of resistance training as a key component of lifestyle recommendations for diabetes prevention. Long-Term Resistance Training and Risk of Type 2 Diabetes – https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2850563
diabetes risk
How To Reduce Your DM2 Risk 31%
The results, published in Annals of Internal Medicine, were based on 4,746 adults between ages 55 and 75. All had overweight or obesity and metabolic syndrome, but none had diabetes or cardiovascular disease at the start of the study. Researchers followed participants for six years to see whether a more intensive Mediterranean based lifestyle plan could offer stronger protection against type 2 diabetes than the traditional Mediterranean diet alone.
One group followed a calorie reduced Mediterranean diet (about 600 kcal fewer per day), added moderate physical activity (brisk walking, strength and balance training), and received professional guidance. The comparison group followed a traditional Mediterranean diet without calorie restriction or exercise advice.
The difference between the two approaches was striking. Participants in the intervention group were 31% less likely to develop type 2 diabetes than those in the comparison group. Universidad de Navarra. “Scientists found a smarter Mediterranean diet that slashes diabetes risk by 31%.” ScienceDaily. https://www.sciencedaily.com/releases/2026/05/260519003103.htm (accessed May 23, 2026).
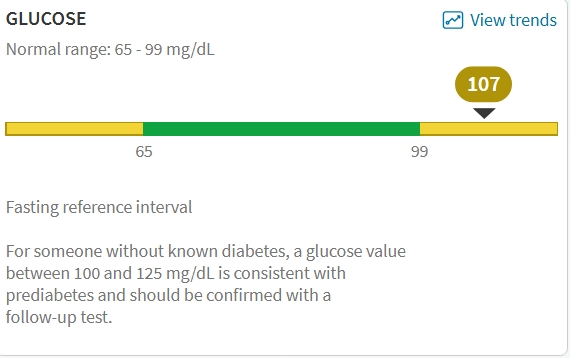
I just had my annual wellness check and got my lab results. All good except my fasting glucose.
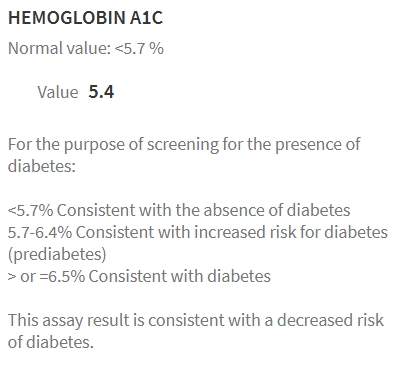
Yikes. Memo to Self, get an A1C. Well, the very next day…
Doc says:
CMP (Comprehensive Metabolic Panel): Your creatinine (a measure related to kidney function) is low, and your blood sugar (glucose) is high; all other values are normal. This test checks how your kidneys and liver are working, your body salts, proteins, and blood sugar. Low creatinine can happen in people with less muscle and may be expected. The slightly high fasting blood sugar could indicate early changes in how your body handles sugar. Options include repeating the blood sugar test next visit.
I know my diet could be better. I know I should eat less, snack less and maybe, just maybe stop drinking beer. But also knowing my IFG is worsening I wondered if there was a diet (besides MedDiet) for IFG?
In recent years, low-calorie diets ranging from 800–1500 kcal/day have gained significant attention in managing type 2 diabetes8,16–19. Studies have shown that low-calorie diets can lead to remission and substantial improvements in cardiometabolic risk factors for a significant proportion of individuals with type 2 diabetes8,16–19. These diets are generally well-tolerated and safe, with only mild side effects reported. Table 1 summarizes the key low-calorie diet studies conducted in people with type 2 diabetes8,16–19. Studies implementing low-calorie diets over a 2–5 month period, primarily high in protein and low in fat, have resulted in a mean weight loss of 7–15 kg (8–15% of initial body weight). This level of weight loss was accompanied by a notable reduction in hepatic fat and improved hepatic insulin sensitivity and first-phase insulin secretion. As a result, fasting plasma glucose levels decreased significantly by 27.8 to 43.2 mg/dL. This suggests that low-calorie diets may also be effective for individuals with i-IFG, as they target the pathophysiological defects characterizing this prediabetes phenotype8,16–19. Figure 1 visually depicts the potential reversal of the twin cycle hypothesis through low-calorie diets in individuals with i-IFG. The twin cycle hypothesis20 postulates that chronic excess calorie intake results in increased accumulation of fat in the liver, leading to resistance against insulin’s suppression of hepatic glucose production. Additionally, excess liver fat increases lipid transportation to the pancreas, impairing β-cell function and further promoting hepatic glucose production. These self-reinforcing cycles between the liver and pancreas ultimately result in the onset of hyperglycemia.
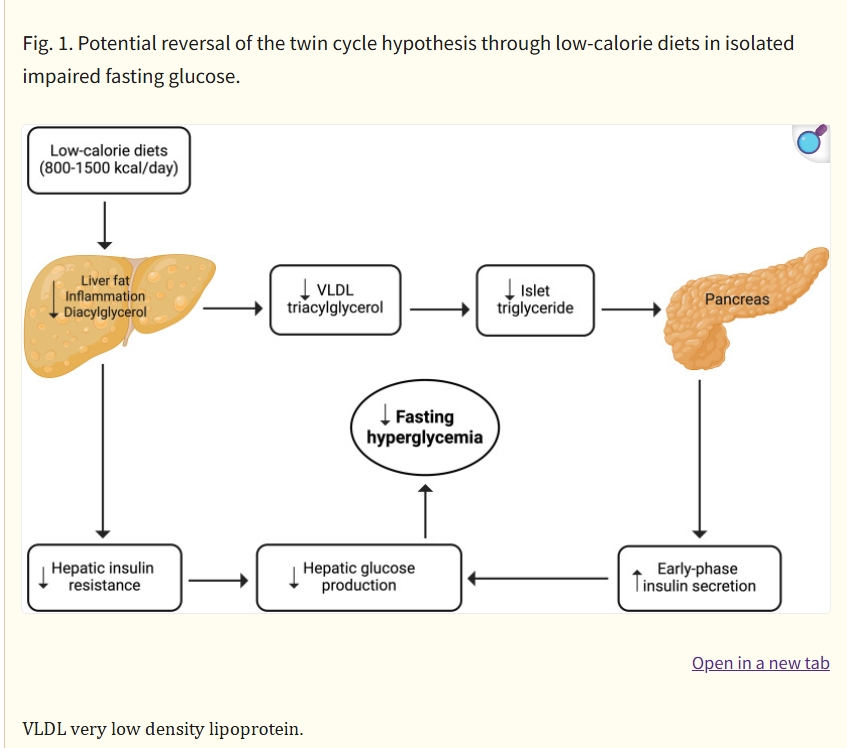
Low-calorie diets for people with isolated impaired fasting glucose – Commun Med (Lond) . 2024 Mar 1;4:35. doi: 10.1038/s43856-024-00466-2
The Plan
- Eat less
- Move more
- Drink less beer
I like to keep things simple.
High Altitude and Diabetes Risk (in mice)
In findings published in Cell Metabolism, the team demonstrated that red blood cells can alter their metabolism when oxygen levels drop. This shift allows the cells to deliver oxygen to tissues more efficiently at high altitude. At the same time, it lowers circulating blood sugar, offering a potential explanation for reduced diabetes risk. Gladstone Institutes. “Scientists discover why high altitude protects against diabetes.” ScienceDaily https://www.sciencedaily.com/releases/2026/02/260221060952.htm (accessed February 21, 2026).
Journal Reference:
- Yolanda Martí-Mateos, Zohreh Safari, Shaun Bevers, Ayush D. Midha, Will R. Flanigan, Tej Joshi, Helen Huynh, Brandon R. Desousa, Skyler Y. Blume, Alan H. Baik, Stephen Rogers, Aaron V. Issaian, Allan Doctor, Angelo D’Alessandro, Isha H. Jain. Red blood cells serve as a primary glucose sink to improve glucose tolerance at altitude. Cell Metabolism, 2026; DOI: 10.1016/j.cmet.2026.01.019
How To Reduce Your Risk of Developing Diabetes
The researchers, from 23 universities in Spain and Harvard Chan School, split 4,746 PREDIMED-Plus participants into an intervention group and a control group and followed their health outcomes for six years. The intervention group adhered to a Mediterranean diet; reduced their caloric intake by about 600 calories per day; engaged in moderate physical activity, such as brisk walking and strength and balance exercises; and received professional support for weight loss control. The control group adhered to a Mediterranean diet without calorie restriction, exercise guidance, or professional support. Participants ranged from age 55 to 75, were overweight or obese, and had metabolic syndrome, but were free of T2D at baseline.
The study found that those in the intervention group had a 31% lower risk of developing T2D compared to those in the control group. Additionally, the intervention group lost an average of 3.3 kilograms and reduced their waist circumference by 3.6 centimeters, compared to 0.6 kilograms and 0.3 centimeters in the control group. Scientists found 3 simple tweaks that cut diabetes risk by 31% – https://www.sciencedaily.com/releases/2025/08/250829022835.htm Harvard T.H. Chan School of Public Health. ScienceDaily. http://www.sciencedaily.com/releases/2025/08/250829022835.htm (accessed August 29, 2025).
Guess I’ll cut out beer.
Another Troubling Trend
The SEARCH data demonstrate an increase in the youth population aged 0-19 diagnosed with type 1 or type 2 diabetes in five representative US centers. Between 2002 and 2018, the annual incidence rose by about 2% per year for type 1 diabetes and 5% per year for type 2 diabetes. The rates of increase for both types were greater among non-White than White youth.
Troubling Trend as Both Diabetes Types Rise Among US Youth – Medscape – Mar 08, 2023. – https://www.medscape.com/viewarticle/989327
Diet and lifestyle until proven otherwise.
Just Another Sweet Saturday Morning
These findings show that the prevalence of food insecurity in the U.S. is highest among Americans for whom a healthy diet is especially critical—Medicaid enrollees with insulin-dependent diabetes and diabetes-related eye or kidney complications (over 40% were food insecure). The problem of co-occurring food insecurity and diabetes among the nation’s disadvantaged has likely worsened during the coronavirus disease 2019 pandemic.
The Prevalence of Food Insecurity Is Highest Among Americans for Whom Diet Is Most Critical to Health — Diabetes Care 2021 Jun; 44(6): e131-e132. https://doi.org/10.2337/dc20-3116
In patients with newly diagnosed T2DM, alcohol abstinence was associated with a low risk of AF development. Lifestyle modifications, such as alcohol abstinence, in patients newly diagnosed with T2DM should be recommended to reduce the risk of AF.
Diabetes Care 2021 Jun; 44(6): 1393-1401. https://doi.org/10.2337/dc20-2607
New research published in Diabetologia has shown that if people achieve and maintain substantial weight loss to manage their type 2 diabetes, many can also effectively control their high blood pressure and stop or cut down on their anti-hypertensive medication.
Diabetologia. “Diabetes remission diet also lowers blood pressure and reduces need for medication.” ScienceDaily. ScienceDaily, 31 May 2021 — https://www.sciencedaily.com/releases/2021/05/210531180422.htm
Sat 6/19
Spice Blend
1 teaspoon ground cumin
1 teaspoon ground coriander
1 teaspoon smoked paprika
½ teaspoon ground turmeric
½ teaspoon dried oregano
½ teaspoon dried chili flakes
¼ teaspoon ground cinnamon
Copied from The First Mess Seven Spice Chickpea Stew recipe https://thefirstmess.com/2016/01/20/vegan-seven-spice-chickpea-stew-recipe/ so I don’t have to look it up online again if I decide to make this dish tonight.
During Pandemic Year One I lost 25 pounds. My PCP was impressed but when I told her how my diet changed she put her “doctor face” on, looked me straight in the eyes and said,
“I can’t wait to see your blood test results.”
Due to my family history my risk of developing DM2 is approximately 25% higher than the average underwriter. When I asked a prominent Endocrinologist for some advice many years ago he too put on his “doctor face” looked me straight in the eyes and said,
“Stay as thin as you can as long as you can.”
Yesterday I went to see Kevin and got a fresh flattop. The first question he asked was,
“Did you lose more weight?”
No, I haven’t. But my face definitely looks thinner without a mask.

BTW my blood work was about the same as last year even with my change in diet.
Preferred Plus NN.
Type 2 Diabetes Risk and…Sardines?
Older people with prediabetes who followed a diet rich in sardines for 1 year show significant reductions in risk of developing type 2 diabetes compared with those placed on a similarly healthy diet but without the sardines, results from a new randomized trial show.
“A 1-year, sardine-enriched type 2 diabetes-preventive diet in an elderly population with prediabetes exerts a greater protective effect against developing type 2 diabetes and cardiovascular events, by improving anthropometric parameters, blood chemistry profile, lipid composition in erythrocytes membranes, and metabolomics data,” report the authors in research published in Clinical Nutrition by Diana Díaz-Rizzolo, PhD, of the Hospital Clinic of Barcelona, Spain, and colleagues.
Sardines Linked to Reduced Type 2 Diabetes Risk — https://www.medscape.com/viewarticle/951528?src=rss#vp_1
Very small study with very interesting findings.
If I only liked sardines.
An Early-Onset Subgroup of Type 2 Diabetes: A Multigenerational, Prospective Analysis in the Framingham Heart Study
Abstract
OBJECTIVE To assess the relation of type 2 diabetes occurring earlier (age <55 years) versus later in life to the risk of cardiovascular death and to diabetes in offspring.
RESEARCH DESIGN AND METHODS In the Framingham Heart Study, a community-based prospective cohort study, glycemic status was ascertained at serial examinations over six decades among 5,571 first- and second-generation participants with mortality data and 2,123 second-generation participants who initially did not have diabetes with data on parental diabetes status. We assessed cause of death in a case (cardiovascular death)–control (noncardiovascular death) design and incident diabetes in offspring in relation to parental early-onset diabetes.
RESULTS Among the participants in two generations (N = 5,571), there were 1,822 cardiovascular deaths (including 961 coronary deaths). The odds of cardiovascular versus noncardiovascular death increased with decreasing age of diabetes onset (P < 0.001 trend). Compared with never developing diabetes, early-onset diabetes conferred a 1.81-fold odds (95% CI 1.10–2.97, P = 0.02) of cardiovascular death and 1.75-fold odds (0.96–3.21, P = 0.07) of coronary death, whereas later-onset diabetes was not associated with greater risk for either (P = 0.09 for cardiovascular death; P = 0.51 for coronary death). In second-generation participants, having a parent with early-onset diabetes increased diabetes risk by 3.24-fold (1.73–6.07), whereas having one or both parents with late-onset diabetes increased diabetes risk by 2.19-fold (1.50–3.19).
CONCLUSIONS Our findings provide evidence for a diabetes subgroup with an early onset, a stronger association with cardiovascular death, and higher transgenerational transmission.
Diabetes Care 2020 Dec; 43(12): 3086-3093. https://doi.org/10.2337/dc19-1758
Translation – The earlier you develop diabetes your risk of CVD and coronary death is higher. An if one or both of your parents developed either early onset or late onset diabetes you’re screwed.
COVID-19 and Diabetes, Sub-types of DM2, B Vitamins in Diabetes Incidence and more
This article provides an overview of the clinical evidence on the poorer clinical outcomes of COVID-19 infection in patients with diabetes versus patients without diabetes, including in specific patient populations, such as children, pregnant women, and racial and ethnic minorities.
COVID-19 and Diabetes: A Collision and Collusion of Two Diseases — Diabetes 2020 Oct; dbi200032. https://doi.org/10.2337/dbi20-0032
In the article above the researchers reviewed nearly 90 studies.

Type 2 diabetes (T2D) is defined by a single metabolite, glucose, but is increasingly recognized as a highly heterogeneous disease, including individuals with varying clinical characteristics, disease progression, drug response, and risk of complications. Identification of subtypes with differing risk profiles and disease etiologies at diagnosis could open up avenues for personalized medicine and allow clinical resources to be focused to the patients who would be most likely to develop diabetic complications, thereby both improving patient health and reducing costs for the health sector. More homogeneous populations also offer increased power in experimental, genetic, and clinical studies. Clinical parameters are easily available and reflect relevant disease pathways, including the effects of both genetic and environmental exposures. We used six clinical parameters (GAD autoantibodies, age at diabetes onset, HbA1c, BMI, and measures of insulin resistance and insulin secretion) to cluster adult-onset diabetes patients into five subtypes. These subtypes have been robustly reproduced in several populations and associated with different risks of complications, comorbidities, genetics, and response to treatment. Importantly, the group with severe insulin-deficient diabetes (SIDD) had increased risk of retinopathy and neuropathy, whereas the severe insulin-resistant diabetes (SIRD) group had the highest risk for diabetic kidney disease (DKD) and fatty liver, emphasizing the importance of insulin resistance for DKD and hepatosteatosis in T2D. In conclusion, we believe that subclassification using these highly relevant parameters could provide a framework for personalized medicine in diabetes.
Subtypes of Type 2 Diabetes Determined From Clinical Parameters — Diabetes 2020 Oct; 69(10): 2086-2093. https://doi.org/10.2337/dbi20-0001
Not just potential for personalized medicine in the treatment of diabetes but perhaps a framework for better risk stratification and selection in life insurance.
Intakes of Folate, Vitamin B6, and Vitamin B12 in Relation to Diabetes Incidence Among American Young Adults: A 30-Year Follow-up Study
RESULTS During 30 years (mean 20.5 ± 8.9) of follow-up, 655 incident cases of diabetes occurred. Intake of folate, but not vitamin B6 or vitamin B12, was inversely associated with diabetes incidence after adjustment for potential confounders. Compared with the lowest quintile of total folate intake, the multivariable-adjusted hazard ratios (95% CI) in quintiles 2–5 were 0.85 (0.67–1.08), 0.78 (0.60–1.02), 0.82 (0.62–1.09), and 0.70 (0.51–0.97; Ptrend = 0.02). Higher folate intake was also associated with lower plasma homocysteine (Ptrend < 0.01) and insulin (Ptrend < 0.01). Among supplement users, folate intake was inversely associated with serum C-reactive protein levels (Ptrend < 0.01).
CONCLUSIONS Intake of folate in young adulthood was inversely associated with diabetes incidence in midlife among Americans. The observed association may be partially explained by mechanisms related to homocysteine level, insulin sensitivity, and systemic inflammation.
Intakes of Folate, Vitamin B6, and Vitamin B12 in Relation to Diabetes Incidence Among American Young Adults: A 30-Year Follow-up Study — Diabetes Care 2020 Oct; 43(10): 2426-2434. https://doi.org/10.2337/dc20-0828
Folate is a B vitamin that occurs naturally in foods such as green leafy vegetables, citrus fruit, and beans. So eat your greens and beans. Taking a supplement can’t hurt either. My multivitamin has plenty of folate.
Metformin Should Not Be Used to Treat Prediabetes
Based on the results of the Diabetes Prevention Program Outcomes Study (DPPOS), in which metformin significantly decreased the development of diabetes in individuals with baseline fasting plasma glucose (FPG) concentrations of 110–125 vs. 100–109 mg/dL (6.1–6.9 vs. 5.6–6.0 mmol/L) and A1C levels 6.0–6.4% (42–46 mmol/mol) vs. <6.0% and in women with a history of gestational diabetes mellitus, it has been suggested that metformin should be used to treat people with prediabetes. Since the association between prediabetes and cardiovascular disease is due to the associated nonglycemic risk factors in people with prediabetes, not to the slightly increased glycemia, the only reason to treat with metformin is to delay or prevent the development of diabetes. There are three reasons not to do so. First, approximately two-thirds of people with prediabetes do not develop diabetes, even after many years. Second, approximately one-third of people with prediabetes return to normal glucose regulation. Third, people who meet the glycemic criteria for prediabetes are not at risk for the microvascular complications of diabetes and thus metformin treatment will not affect this important outcome. Why put people who are not at risk for the microvascular complications of diabetes on a drug (possibly for the rest of their lives) that has no immediate advantage except to lower subdiabetes glycemia to even lower levels? Rather, individuals at the highest risk for developing diabetes—i.e., those with FPG concentrations of 110–125 mg/dL (6.1–6.9 mmol/L) or A1C levels of 6.0–6.4% (42–46 mmol/mol) or women with a history of gestational diabetes mellitus—should be followed closely and metformin immediately introduced only when they are diagnosed with diabetes.
Metformin Should Not Be Used to Treat Prediabetes — Diabetes Care 2020 Sep; 43(9): 1983-1987. https://doi.org/10.2337/dc19-2221

You must be logged in to post a comment.