The results, published in Annals of Internal Medicine, were based on 4,746 adults between ages 55 and 75. All had overweight or obesity and metabolic syndrome, but none had diabetes or cardiovascular disease at the start of the study. Researchers followed participants for six years to see whether a more intensive Mediterranean based lifestyle plan could offer stronger protection against type 2 diabetes than the traditional Mediterranean diet alone.
One group followed a calorie reduced Mediterranean diet (about 600 kcal fewer per day), added moderate physical activity (brisk walking, strength and balance training), and received professional guidance. The comparison group followed a traditional Mediterranean diet without calorie restriction or exercise advice.
The difference between the two approaches was striking. Participants in the intervention group were 31% less likely to develop type 2 diabetes than those in the comparison group. Universidad de Navarra. “Scientists found a smarter Mediterranean diet that slashes diabetes risk by 31%.” ScienceDaily. https://www.sciencedaily.com/releases/2026/05/260519003103.htm (accessed May 23, 2026).
I just had my annual wellness check and got my lab results. All good except my fasting glucose.
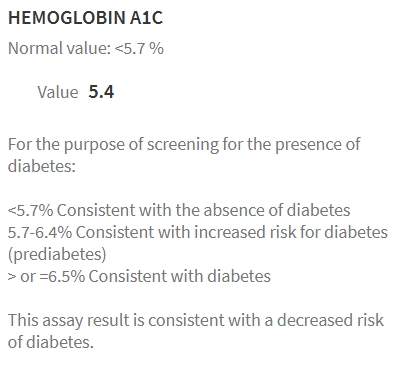
Yikes. Memo to Self, get an A1C. Well, the very next day…
Doc says:
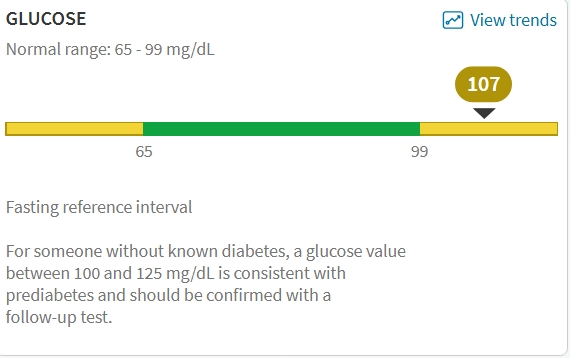
CMP (Comprehensive Metabolic Panel): Your creatinine (a measure related to kidney function) is low, and your blood sugar (glucose) is high; all other values are normal. This test checks how your kidneys and liver are working, your body salts, proteins, and blood sugar. Low creatinine can happen in people with less muscle and may be expected. The slightly high fasting blood sugar could indicate early changes in how your body handles sugar. Options include repeating the blood sugar test next visit.
I know my diet could be better. I know I should eat less, snack less and maybe, just maybe stop drinking beer. But also knowing my IFG is worsening I wondered if there was a diet (besides MedDiet) for IFG?
In recent years, low-calorie diets ranging from 800–1500 kcal/day have gained significant attention in managing type 2 diabetes8,16–19. Studies have shown that low-calorie diets can lead to remission and substantial improvements in cardiometabolic risk factors for a significant proportion of individuals with type 2 diabetes8,16–19. These diets are generally well-tolerated and safe, with only mild side effects reported. Table 1 summarizes the key low-calorie diet studies conducted in people with type 2 diabetes8,16–19. Studies implementing low-calorie diets over a 2–5 month period, primarily high in protein and low in fat, have resulted in a mean weight loss of 7–15 kg (8–15% of initial body weight). This level of weight loss was accompanied by a notable reduction in hepatic fat and improved hepatic insulin sensitivity and first-phase insulin secretion. As a result, fasting plasma glucose levels decreased significantly by 27.8 to 43.2 mg/dL. This suggests that low-calorie diets may also be effective for individuals with i-IFG, as they target the pathophysiological defects characterizing this prediabetes phenotype8,16–19. Figure 1 visually depicts the potential reversal of the twin cycle hypothesis through low-calorie diets in individuals with i-IFG. The twin cycle hypothesis20 postulates that chronic excess calorie intake results in increased accumulation of fat in the liver, leading to resistance against insulin’s suppression of hepatic glucose production. Additionally, excess liver fat increases lipid transportation to the pancreas, impairing β-cell function and further promoting hepatic glucose production. These self-reinforcing cycles between the liver and pancreas ultimately result in the onset of hyperglycemia.
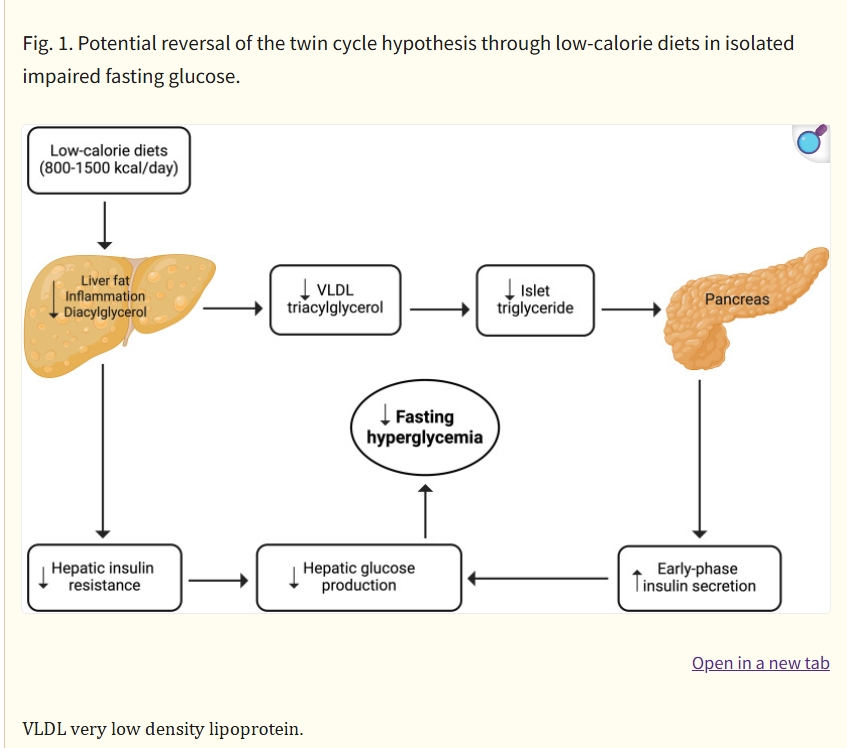
Low-calorie diets for people with isolated impaired fasting glucose – Commun Med (Lond) . 2024 Mar 1;4:35. doi: 10.1038/s43856-024-00466-2
The Plan
- Eat less
- Move more
- Drink less beer
I like to keep things simple.

You must be logged in to post a comment.