As of Sept. 18, there have been at least 39,000 reported positive cases tied to meatpacking facilities in at least 419 plants in 40 states, and at least 185 reported worker deaths in at least 51 plants in 27 states.
And in case you missed this interesting hypothesis…
Our laboratory work has shown that SARS-CoV-2 can survive the time and temperatures associated with transportation and storage conditions associated with international food trade. When adding SARS-CoV-2 to chicken, salmon and pork pieces there was no decline in infectious virus after 21 days at 4°C (standard refrigeration) and –20°C (standard freezing).
The swift action of the government slowed the spread of the virus and bought the country vital time to prepare its hospitals and testing system, says the team of scientists advising it. It also meant they could stop the virus’s spread before it became exponential as it did in the hardest hit nations.
“By acting really fast we were able to completely identify and stop the transmission chain of the disease in every [outbreak],” says Rafael Radi, a biochemist at Montevideo’s University de la Republica leading the government’s advisory group.
Epidemiologists traced the first outbreak to a wedding, where all attendees were tested and suspected infections isolated within 24 hours. The same approach was employed at the three subsequent outbreaks: a mental health care hospital, a care home for the elderly, and the city of Rivera, bordering Brazil. The result was that most local transmission chains have been controlled at the second or third ration of contacts,4 before their spread accelerated
Oklahoma ranks No. 5 in the U.S. for new COVID-19 cases and test positivity, according to the latest White House Coronavirus Task Force weekly report released Wednesday afternoon. The state’s rate of new weekly cases was 142 per 100,000 people, nearly doubling the U.S. average of 74 per 100,000 people. Its test positivity rate was at 10%, which is more than double the national average of 4.8%.
CVCT CardioBrief published online earlier this week a letter from a group of “clinicians, researchers and imaging specialists” who are concerned about the “presentation, interpretation and media coverage of the role of cardiac magnetic resonance imaging in the management of asymptomatic patients recovered from COVID-19.” It’s short and sweet but makes many excellent points. Let’s…
We do not, as these numbers show, live in one economy. We are a tale of too many economies. There are no one-size fits all solutions, though several trillion dollars more of spending surely will benefit everyone. No part of the country is unaffected by the past months, but some parts are devastated and others merely dented. A sense that we are actually all in this together would dictate that we only thrive when most of us thrive, but that sense was not prevalent enough before this crisis for it to be demonstrable during. Instead, our many economies are making collective stories impossible and added to the sense of fracture that the presidential election and pandemic are magnifying.
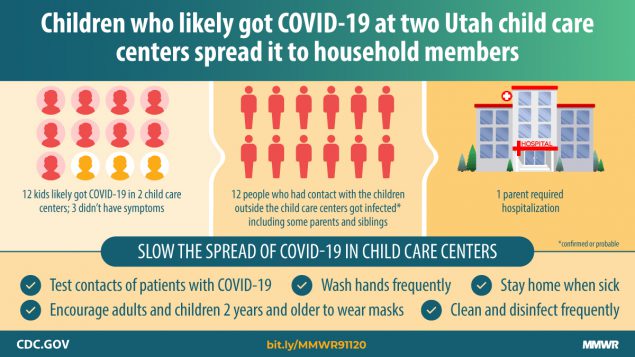
Twelve children acquired COVID-19 in child care facilities. Transmission was documented from these children to at least 12 (26%) of 46 nonfacility contacts (confirmed or probable cases). One parent was hospitalized. Transmission was observed from two of three children with confirmed, asymptomatic COVID-19.
According to a new report commissioned by the Food Research and Action Center (FRAC), as of July, the number of people who said they sometimes or often did not have enough to eat has skyrocketed to 29 million, or 11 percent of adults in the United States. (By comparison, 8 million adults, or around 4 percent, did not have enough to eat in 2018.) In 38 states and Washington, D.C., more than one in ten adults with children had inadequate amounts of food, with the highest rates of hunger in Mississippi, Louisiana, and Texas…
Now, new data from the Census Bureau, referenced in the report, shows that even America’s middle class is now reckoning with hunger. Two years ago, only 3 percent of adults earning between $50,000 and $75,000 a year said they did not have enough to eat; during the pandemic, that rose to 8 percent. Similarly, 5 percent of adults earning between $35,000 and $50,000 reported that hunger in 2018; now, it is 12 percent.
When people envision social distancing, they typically think about the “6-foot rule.”
It’s true that staying 6 feet from other people can reduce the chance of a coronavirus-laden respiratory droplet landing in your eyes, nose or mouth when someone coughs. Most of these droplets are too tiny to see, and people are expelling them into the air all the time – when they shout, talk or even just breathe.
But the 6-foot rule doesn’t account for all risks, particularly indoors.
Think about walking into a room where someone is smoking a cigarette. The closer you are to the cigarette, the stronger the smell – and the more smoke you’re inhaling. That smoke also lingers in the air. Over time, it won’t matter where you are in the room; the smoke will be everywhere.
As professorswho studyfluid dynamics and aerosols, we have been exploring how COVID-19 circulates and the risks it creates. The 6-foot rule is a good benchmark that’s easy to remember, but it’s important to understand its limitations.
Aerosols and an 86-year-old rule
The 6-foot rule goes back to a paper published in 1934 by William F. Wells, who was studying how tuberculosis spreads. Wells estimated that small respiratory droplets evaporate quickly, while large ones rapidly fall to the ground, following a ballistic-like trajectory. He found that the farthest any droplets traveled before either settling or evaporating was about 6 feet.
While that distance can reduce exposure, it does not provide a complete picture of infection risk from the SARS-CoV-2 virus.
When people exhale, they expel respiratory droplets with a wide range of sizes. Most are smaller than 10 microns in diameter. These can quickly decrease to approximately 40% of their original diameter, or smaller, due to evaporation.
The droplets will not completely evaporate, however. This is because they consist of both water and organic matter, potentially including the SARS-CoV-2 virus. These tiny droplets stay suspended in the air for minutes to hours, posing a risk to anyone who comes into contact with them. When suspended in the air, these droplets are commonly referred to as aerosols.
Indoors or outdoors: Ventilation matters
Infection risk is highest right next to a person who has the virus and decreases with distance. However, the way respiratory droplets mix in the air and the resulting concentration influence the distance needed to safely avoid exposure.
Outdoors, the combination of physical distancing and face coverings provides excellent protection against virus transmission. Think again of being near a smoker. Smoke can be carried by the wind much farther than 6 feet, but high concentrations of smoke do not usually build up outdoors because the smoke is quickly diluted by the large volume of air. A highly effective strategy to avoid breathing smoke is to avoid being directly downwind of the smoker. This is also true for respiratory droplets.
Indoors, the picture is very different.
Very light room air currents from fans and ventilation units can transport respiratory droplets over distances much greaterthan 6 feet. However, unlike being outdoors, most indoor spaces have poor ventilation. That allows the concentration of small airborne respiratory droplets to build up over time, reaching all corners of a room.
When indoors, the infection risk depends on variables such as the number of people in the room, the size of the room and the ventilation rate. Speaking loudly, yelling or singing can also generate much larger concentrations of droplets, greatly increasing the associated infection risk.
In pre-COVID-19 times, few people worried about respiratory infection from small virus-laden droplets accumulating indoors because their virus load was usually too low to cause an infection.
There is no safe distance in a poorly ventilated room, unfortunately. Good ventilation and filtration strategies that bring in fresh air are critical to reduce aerosol concentration levels, just as opening windows can clear out a smoke-filled room.
In addition, masks or face coverings should be worn at all times in public indoor environments. They both reduce the concentration of respiratory droplets being expelled into the room and provide some protection against inhaling infectious aerosols.
The 6-foot social distancing guideline is a critical tool for combating the spread of COVID-19. However, as more activities move indoors with the arrival of cooler weather this fall, implementing safeguards, including those you might use to avoid inhaling cigarette smoke, will be essential.
I mentioned in my post entitled “Should You Utilize A Home Pulse Oximeter During COVID-19?” that I had purchased a home pulse oximeter and had used it to monitor my oxygen saturation (SpO2) levels during the time I had COVIDesque symptoms recently. Personally, I felt the device was returning accurate information and was helpful in…
And if you decide not to read Dr. Pearson’s entire article here’s your take home message:
During my illness I would measure my SpO2 twice daily and at times when I felt short of breath. When I felt the worst I noted the SpO2 had dropped to 95%. Within 24 hours it rebounded and I recorded >96% thereafter.
If the SpO2 had progressively dropped and consistently showed values <90% I would have contacted my primary care physician and described the constellation of signs (pulse rate, respiratory rate, BP, and SpO2) and symptoms (shortness of breath, cough, headache, fatigue, etc.) that I had and seek his advice on what to do
Oklahoma has an 11.3% positivity rate — the percentage of COVID-19 tests that are positive — more than double the country’s positivity rate of 5.2%. The state’s rate is its highest yet, surpassing the 10.1% in the July 26 report to become the second time Oklahoma has landed in the positivity red zone.
Oklahoma’s new case rate is 146 per 100,000 people, nearly two-thirds more than the national average of 88 per 100,000. The state has been in the red zone for new cases for nine consecutive weeks.
A week ago the report warned that virus transmission was increasing in the “major university towns.”




You must be logged in to post a comment.